Epilepsy Guide
Skip surgery
😏cidpusa.org
Epilepsy may present as a symptom of many neurological disorders and often an etiological explanation cannot be identified.There is growing evidence that autoimmune mechanisms might have a role in most patients. This includes numerous reports of the detection of theoretically relevant serum autoantibodies, experimental data showing that antibodies can be epileptogenic, and a responseof many epilepsy syndromes to immunomodulation by IVIG and steroids to full recovery.
The evidence for immunological mechanisms in epilepsy can be examined within the following three main areas: the childhood epilepsy syndromes, epilepsy associated with other immunologically mediated diseases, and the more common unselected groups of patients with epilepsy.
Our researchers started with research work at the NIH in epilepsy . Soon we found out that we were not going to refer patients for epilepsy surgery. As the patients started to respond to autoimmune treatments. Every epilepsy patient should go on a gluten free diet due to possibility of Celiac disease. Only if the patient does not respond to this diet a search for viruses should be done.
Today with a external electrical stimulator like TENS or Zapper can stop the seizures in any animal or human by destroying the viruses which are causing the inflammation. Even spices like turmeric are effective in stopping seizures and epilepsy as they reduce inflammation.
An estimated 0.5−1% of the world population is epileptic, with completely autoimmune causes and no effective treatment. Epilepsies have long been viewed as diseases of the central nervous system (CNS), but in recent years, evidence has mounted that all may actually be autoimmune-mediated. If so, the way we regard and treat these epilepsies may require a revolutionary change.
We have treated many patients with a external electrical stimulator which has helped control epilepsy. If you want to purchase the unit or need more info please read our E-book for full details in the electronic section. You can also use FDA approved TENS units to help your seizures . This circuit given to any electronic shop can be built for $1 in any country of the world.
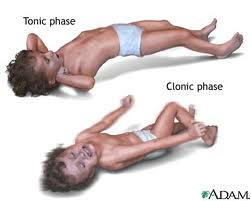 The first clue to the autoimmune nature of some epilepsies
is by a sudden onset of uncontrolled behaviour lasting a few seconds
followed by extreme fatigue or sleep.
Scientific research confirms the presence of antibodies to a major excitatory
neurotransmitter in the CNS. Antibodies to this particular
glutamate receptor, one of the subtypes (GluR3), have now
been found in three severe human epilepsies: Rasmussen's
encephalitis (RE), noninflammatory focal epilepsy and
"catastrophic" epilepsy. Epileptic RE patients harbor a kaleidoscope of non-GluR3
antibodies, although surgical removal of the epileptic loci only
reduces the concentration of antibodies to GluR3B in the serum
and cerebrospinal fluid (CSF), pointing to their special
relevance . Finally, a proportion of patients with
seizures, cognitive changes and sleep disorders (limbic
syndromes) or epilepsy associated with Hashimoto's or viral
encephalitis harbor autoantibodies against voltage-gated
potassium channels.
The first clue to the autoimmune nature of some epilepsies
is by a sudden onset of uncontrolled behaviour lasting a few seconds
followed by extreme fatigue or sleep.
Scientific research confirms the presence of antibodies to a major excitatory
neurotransmitter in the CNS. Antibodies to this particular
glutamate receptor, one of the subtypes (GluR3), have now
been found in three severe human epilepsies: Rasmussen's
encephalitis (RE), noninflammatory focal epilepsy and
"catastrophic" epilepsy. Epileptic RE patients harbor a kaleidoscope of non-GluR3
antibodies, although surgical removal of the epileptic loci only
reduces the concentration of antibodies to GluR3B in the serum
and cerebrospinal fluid (CSF), pointing to their special
relevance . Finally, a proportion of patients with
seizures, cognitive changes and sleep disorders (limbic
syndromes) or epilepsy associated with Hashimoto's or viral
encephalitis harbor autoantibodies against voltage-gated
potassium channels. All these autoimmune epilepsy conditions can easily be treated with IVIG. INTRA VENOUS IMMUNE GLOBULIN HELPS RECUE INFLMMATION IN AUTOIMMUNE DISEASES AND ALSO REUCES THE VIRAL LOADS.
All insurances in USA can cover IVIG for encephalitis and epilepsy.
Autoimmune conditions like Stiff person syndrome are assossiated with epilepsy and agin covered for IVIG rx by all insurances.
continue to next page
😏