MYASTHENIA GRAVIS
A Holistic Therapy
Neurological manifestations of Myasthenia Gravis,
Walter Last
.Check our E-BOOK alternative treatment guide
Read re Skin Vitamin By Walter Last see the Thymus Gland below
Severe muscle weakness becomes increasingly more common in recent times. The classical disease with severe muscle weakness is myasthenia gravis or M.G. It is most common in young women, although it may develop at any age and in both sexes. Males are more affected in their later decades of life.
Certain muscles become chronically weak and easily fatigued. Most affected are the muscles of the head and neck, later progressively also the muscles of the chest and limbs. The first sign of myasthenia gravis is usually a drooping eyelid (ptosis). Frequently double vision (diplopia) develops as the disease progresses, also difficulty chewing or swallowing or even breathing. The speech may be slurred and the vision blurred. Usually the condition becomes worse as the day progresses.
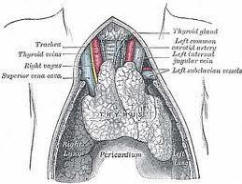
In medical treatment a group of drugs, called anticholinesterases, is used, such as neostigmine or pyridostigmine. These delay the normal inactivation of the neurotransmitter acetylcholine, which results in a temporary improvement in muscle functions. Frequently the thymus gland is greatly enlarged and may be surgically removed. This can result in some medium-term improvement in one-third of cases.
There are frequent side effects from drug therapy, such as abdominal cramps, diarrhoea, nausea, vomiting, excessive mucus formation, bronchial spasms, twitching of face muscles, spasms and freezing of muscles, tremors, in coordination and paralysis. It is easy to overdose with a resulting 'cholinergic' crisis often resulting in death.
Removal of the thymus results in complete healing in 80% of the cases but in some disturbances of the calcium and manganese metabolism, it greatly weakens the immune system and perpetuates the muscle weakness which then does not respond any more to biological therapy.
CAUSES OF MYASTHENIA GRAVIS
Myasthenia has droopy eyelids
Myasthenia gravis has been shown to be an autoimmune disease. This means that the immune system attacks some of its own body proteins. Specifically, the transmission of signals from the nerve endings to the muscle receptors is partly blocked by antibodies. The messenger chemical or neurotransmitter released as signal from nerve endings to muscles is acetylcholine. Acetylcholine molecules travel the short distance in the gapbetween nerve ending and muscle to find a receptor on the motor end plate. When a sufficient number of acetylcholine molecules are attachedto muscle receptors, there is an electric discharge of the normal membrane potential and the muscle fibre can contract.
In myasthenia gravis many or most of the receptors are already occupied by antibodies, therefore, not enough acetylcholine molecules find receptors to trigger this discharge and subsequent muscle contraction. Normally, the acetylcholine is split by an enzyme and, with this, removedfrom the receptor in a fraction of a second. Using drugs, which hinder this enzyme, acetylcholine molecules have more time to find receptors with an increased chance to lead to a discharge.
Please continue to next page the role of fluoride & nutritional factors in Myasthenia