Search CIDPUSA WEBSITE
INSULINOMA
An insulinoma is a neuroendocrine tumor. An insulinoma is a neuroendocrine tumor deriving mainly from pancreatic islet cells that produce excessive amounts of insulin. About 90% of insulinomas are benign. In healthy individuals, insulin and C-peptide are secreted in equimolar quantities because they derive from the same inactive precursor, proinsulin. Normally, less than 20% of proinsulin is released directly into the circulation.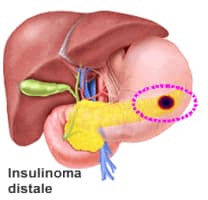
Some insulinomas secrete additional hormones, such as gastrin, 5-hydroxyindolic acid, adrenocorticotropic hormone (ACTH), glucagon, human chorionic gonadotropin, and somatostatin. The tumor may secrete insulin in short bursts, causing wide fluctuations in blood insulin levels
Frequency
United States
Insulinomas are the most common pancreatic endocrine tumor. The incidence is 4 cases per million people per year. These make up 55% of neuroendocrine tumors, as stated above in Background
Age
- The median age at diagnosis is about 47 years, except in insulinoma patients with MEN 1, in whom the median age is the mid 20s.
- In one series, patients with benign disease were younger (mean age of 38 y) than those with metastases (mean age of 52 y).
- Symptoms caused by effects of local tumor mass are very rare.
- About 85% of patients present with symptoms of hypoglycemia with diplopia, blurred vision, palpitations, or weakness.
- Other symptoms include confusion, abnormal behavior, unconsciousness, or amnesia.
- About 12% of patients have grand mal seizures.
- Adrenergic symptoms (hypoglycemia causes adrenalin release) include weakness, sweating, tachycardia, palpitations, and hunger.
- Symptoms may be present from 1 week to as long as several decades prior to the diagnosis (1 mo to 30 y, median 24 mo, as found in a large series of 59 patients).
- Hypoglycemia usually occurs several hours after a meal.
- In severe cases, symptoms may develop in the postprandial period. Symptoms can be aggravated by exercise, alcohol, hypocaloric diet, and treatment with sulfonylureas.
- Weight gain occurs in 20-40% of patients.
Physical
Insulinomas are characterized clinically by the Whipple triad (which occurred in 75% of 67 insulinoma patients as reported recently).
- Episodic hypoglycemia
- Central nervous system (CNS) dysfunction temporally related to hypoglycemia (confusion, anxiety, stupor, convulsions, coma)
- Dramatic reversal of CNS abnormalities by glucose administration
- CONTINUE TO AUTOIMMUNE Hypoglycemia 😏