Search CIDPUSA WEBSITE
EMG NCV |JULY 4, 2020
b) The needle examination
An electrode is introduced into the muscle and recordings are made with mild to moderate activation of the muscle. This test is accompanied by some discomfort, but if performed appropriately should not be torture!
Depolarization of muscle fibers in close proximity to the needle electrode will be recorded as motor unit potentials (MUPs; compare with CMAPs!). A normal muscle and a normal MUP are shown in figure 13.
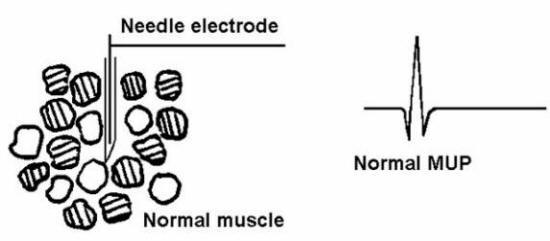
Figure 13 Normal muscle. The above muscle fibers are innervated by three different lower (alpha) motor neurons. Think of the MUP as representing the action potentials of the muscle fibers associated with one of these motor neurons (a motor unit). For example a slight contraction of the muscle during a movement will fire all of the "clear fibers" above, but neither of the "striped fiber" groups.
By analyzing the size of the MUPs (mostly the amplitude and duration), we can make a distinction between diseases that are primarily myopathic (disease of the muscle) versus those which result from denervation. As described in the section on the anatomy of muscle fibers, the muscle fibers innervated by one anterior horn cell / motor axon are spread over 10 - 15 mm of the muscle. Furthermore, the territory innervated by adjacent anterior horn cells overlap so that adjacent muscle fibers are normally innervated by different anterior horn cells or motor axons. With damage to an anterior horn cell or a motor axon the denervated muscle fibers usually become reinnervated by another motor axon with the result that more muscle fibers are innervated by the same anterior horn cell or motor axon in close proximity to the EMG needle. This is seen histologically as type grouping as shown in figure 7. In simplified terms this results in larger MUPs ("neurogenic" MUPs), figure 14. You might wonder why, if there is reinnervation (or "sprouting") and larger MUPs, why are the CMAPs smaller? Well, that is because muscle fibers are also dying (remember group atrophy?)
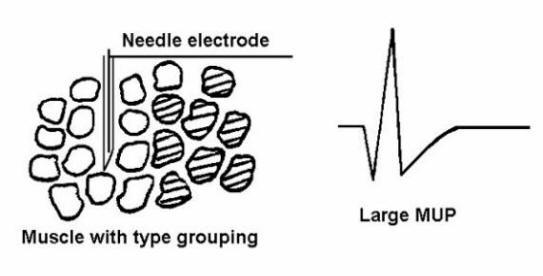
Figure 14 Neurogenic atrophy with type grouping. A large MUP is recorded. Think about the single active motor neuron in Figure 13 as innervating more muscle fibers. When it fires there will be more muscle fiber action potentials and thus a larger MUP.
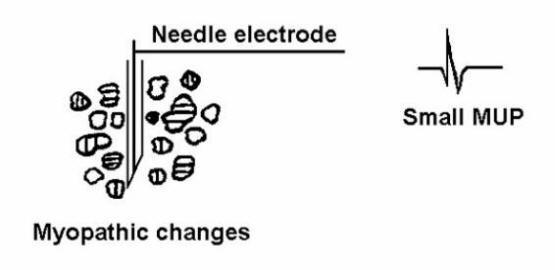
On the other hand in a primary muscle disease, there is loss of muscle fibers, or muscle fibers have a smaller mean diameter than normal, resulting in small MUPs ("myopathic" MUPs), figure 15.
Fasciculations are noted clinically as a contraction of a small group of muscle fibers. They result from the spontaneous discharge of an anterior horn cell or a motor axon with the subsequent contraction of all the muscle fibers innervated by that anterior horn cell or motor axon. Fasciculations can also be recorded with the needle electrode. Clinically, fasciculations are seen after reinnervation of muscle fibers and they are particularly common in amyotrophic lateral sclerosis (motor neuron disease).
Please continue to EMG report next page
65