Search Cidpusa web
Ankylosing Spondylitis
ANKYLOSING SPONDYLITIS
(REACTIVE ARTHRITIS OF THE SPINE)
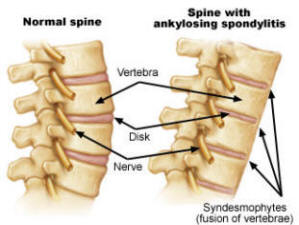
If your back is stiff and hurts when you move, if it hurts to touch two points at the side of the top of your pelvis where it joins your spine (the sacroiliac joint), and if your back x ray shows signs of this disease, you probably suffer from ankylosing spondylitis. You may also have pain and swelling in your eyes, lungs, and heart valves. Most doctors think that ankylosing spondylitis is an autoimmune disease in which a person's immunity is so stupid that it attacks and destroys the joints in his back, rather than just doing its job of protecting a person from infection. They treat you with immune suppressants that may make you feel better, but increase your risk for infections and cancers and shorten your life. Nobody really knows why you have this condition, but the overwhelming evidence is that you inherited your susceptibility from your parents and you got this condition from an infection.
When you are infected, your body protects you by making proteins called antibodies and cells called white blood cells that attack and kill the bacteria. Your immunity recognizes each specific germ by the structure of its surface membranes. Ninety percent of people with ankylosing spondylitis have a gene called HLA-B27, which means that their cells have surface membranes that are like the surface membranes on many bacteria, particularly those that grow and live in your intestinal tract. So, if certain bacteria get into your bloodstream, your immunity recognizes these germs by their surface membranes and makes antibodies and cells that attack and kill them. However, if the cells in your body have similar surface membranes, your own immunity can be fooled and think that you are the invading germ and attack and kill your own cells.
There is one more piece to the puzzle. All people with ankylosing spondylitis have changes in their intestines that look like a disease called Crohn's disease in which they develop bloody ulcers in their intestines and sometimes terrible cramping and diarrhea. If intestinal bacteria are to cause ankylosing spondylitis, they have to have a way to get into the bloodstream, and the intestinal ulcers of Crohn's disease could be the portal of entry.
Hundreds of reports in the literature show that arthritis follows infections with bacteria such as Salmonella that causes typhoid fever , chlamydia that causes burning on urination, and a host of germs that cause diarrhea. Dr. Taurog showed that HLA-B27 rats that are raised in a completely germ-free environment do not develop arthritis or Crohn's disease. This implies that people who have the HLA-B27 surface protein on their cells will not get ankylosing spondylitis or Crohn's disease unless they are infected with certain types of germs.
Reactive arthritis is another type of arthritis that is associated with HLA-B27 genes. It occurs after venereal infections, usually chlamydia. and diarrhea caused by Yersinia or campylobacter. The most promising research going on right now is looking for specific bacteria that have been shown to cause arthritis, and then learn how to protect the body from overreacting to these bacteria, such as Mycobacterium paratuberculosis (that is thought to cause Crohn's disease), paramyxovirus (the measles viruses), Listeria monocytogenes (that causes diarrhea), and abnormal E. Coli that are in your intestines.
Several papers support an infections with mycoplasma, chlamydia and ureaplasma . Virtually all patients have ulcers or changes in their gut similar to those seen in Crohn's disease . Sufferers often have high blood levels of IGG and IGA antibodies that the body produces to kill Klebsiella bacteria which normally live in the intestines of healthy people . Living with a person with ankylosing spondylitis increases your risk for developing the disease.
The surface structure of Klebsiella contains two molecules similar to that of a genetic marker for ankylosing spondylitis called HLA-B27; so does another gut bacteria called bacteroides (6A). When the pain is severe, large amounts of Klebsiella are found in stool samples, and those with ankylosing spondylitis often have intestinal ulcers in the end of the small intestine. A low starch diet that reduces the concentration of klebsiella has been reported to alleviate the back pain (7). Ankylosing spondylitis has been associated with campylobacter, clostridium, salmonella, shigella, yersinia, bacteroides and klebsiella (16).
. I have successfully treated several Crohn's disease patients with a regimen of doxycycline 100 mg twice a day continuously, and metronidazole 250 mg four times a day on alternate weeks, for as long as six months. However, I have not had this success with patients with ankylosing spondylitis. We need research to see if the antibiotic that can kill mycobacterium paratuberculosis that may be the cause of Crohn's disease, will also help control ankylosing spondylitis. In that case, a study should be done to see if clarithromycin, 500 mg twice a day for many months, will help control this condition. The theory that antibiotics may have a role in treatment of Crohn's disease and ankylosing spondylitis is highly controversial and not accepted by most doctors; check with your doctor.
One last point: very often the severe back pain of ankylosing spondylitis can be controlled by taking bisphosphonate drugs that are used to strengthen bones in people who have osteoporosis (18). An exciting study from the University of Alberta in Canada shows that intravenous infusion of pamidronate, a common drug for strengthening bones, helps to control ankylosing spondylitis. Pamidronate is a drug that is used to treat osteoporosis and is safer than most of the drugs used to treat ankylosing spondylitis. The doctor puts around 60 mg of Pamidronate into 500 cc of fluid and runs it into the veins slowly over 4 to 6 hours. When this is done once a week for several weeks, the pains of ankylosing spondylitis often goes away (28)
For treatment see the link on antibiotics and arthritis in the links column
AUTOIMMUNE EPIDEMICTreatment of alcoholic poly neuropathy want to learn about the brain and spinal cord
😏