cidpusa.org
|
;Global Health Help & information Welcome to cidpusa.org |
||
| Guide to natural treatment of all diseases Flame within E-book. | ||
|
Definition Acute kidney failure occurs when illness, infection, or injury damages the kidneys. Temporarily, the kidneys cannot adequately remove fluids and wastes from the body or maintain the proper level of certain kidney-regulated chemicals in the bloodstream.
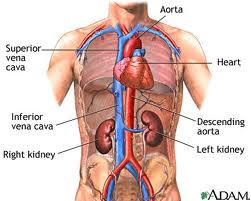
Description The kidneys are the body's natural filtration system. They perform the critical task of processing approximately 200 quarts of fluid in the bloodstream every 24 hours. Waste products like urea and toxins, along with excess fluids, are removed from the bloodstream in the form of urine. Kidney (or renal) failure occurs when kidney functioning becomes impaired. Fluids and toxins begin to accumulate in the bloodstream. As fluids build up in the bloodstream, the patient with acute kidney failure may become puffy and swollen (edematous) in the face, hands, and feet. Their blood pressure typically begins to rise, and they may experience fatigue and nausea. Unlike chronic kidney failure, which is long term and irreversible, acute kidney failure is a temporary condition. With proper and timely treatment, it can typically be reversed. Often there is no permanent damage to the kidneys. Acute kidney failure appears most frequently as a complication of serious illness, like heart failure, liver failure, dehydration, severe burns, and excessive bleeding (hemorrhage). It may also be caused by an obstruction to the urinary tract or as a direct result of kidney disease, injury, or an adverse reaction to a medicine. Causes and symptoms Acute kidney failure can be caused by many different illnesses, injuries, and infections. These conditions fall into three main categories: prerenal, postrenal, and intrarenal conditions. Prerenal conditions do not damage the kidney, but can cause diminished kidney function. They are the most common cause of acute renal failure, and include
Postrenal conditions cause kidney failure by obstructing the urinary tract. These conditions include:
Intrarenal conditions involve kidney disease or direct injury to the kidneys. These conditions include:
Common symptoms of acute kidney failure include
Diagnosis Kidney failure is diagnosed by a doctor. A nephrologist, a doctor that specializes in the kidney, may be consulted to confirm the diagnosis and recommend treatment options. The patient that is suspected of having acute kidney failure will have blood and urine tests to determine the level of kidney function. A blood test will assess the levels of creatinine, blood urea nitrogen (BUN), uric acid, phosphate, sodium, and potassium. The kidney regulates these agents in the blood. Urine samples will also be collected, usually over a 24-hour period, to assess protein loss and/or creatinine clearance. Determining the cause of kidney failure is critical to proper treatment. A full assessment of the kidneys is necessary to determine if the underlying disease is treatable and if the kidney failure is chronic or acute. X rays, magnetic resonance imaging (MRI), computed tomography scan (CT), ultrasound, renal biopsy, and/or arteriogram of the kidneys may be used to determine the cause of kidney failure and level of remaining kidney function. X rays and ultrasound of the bladder and/or ureters may also be needed. | ||
|
|
||